آخر المواضيع المضافة

 النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية
النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
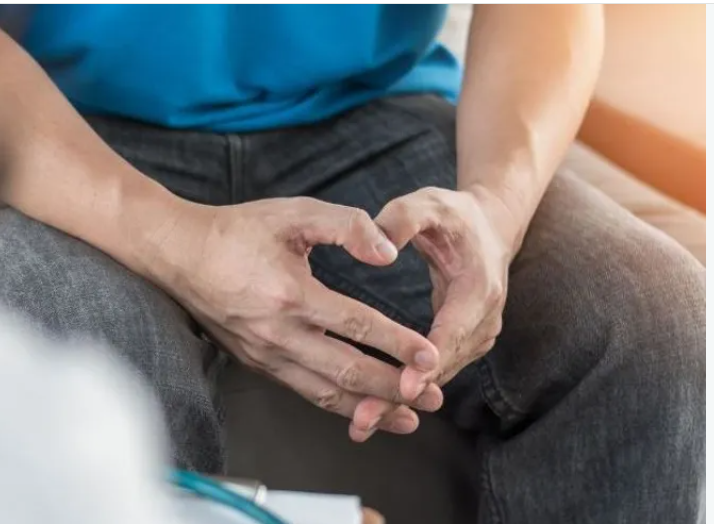
المضادات الحيوية| Unilateral leg swelling |


|
|
Read More
Date: 24-2-2016
Date: 2025-02-09
Date: 2025-03-25
|
Most leg swelling is caused by oedema, the accumulation of fluid within the interstitial space. There are three explanatory mechanisms for development of oedema, which are described in Box 1. Unilateral swelling usually indicates a localised pathology in either the venous or the lymphatic system, while bilateral oedema often represents generalised fluid overload combined with the effects of gravity. However, all causes of unilateral leg swelling may present bilaterally, and generalised fluid over load may present with asymmetrical (and therefore apparently unilateral) oedema. Fluid overload may be the result of cardiac failure, pulmonary hypertension (even in the absence of right ventricular failure), renal failure, hypoalbuminaemia or drugs (calcium channel blockers, glucocorticoids, mineralocorticoids, non-steroidal anti-inflammatory drugs (NSAIDs) and others); for other causes. The remainder of this section focuses on the causes of ‘unilateral’ oedema.

Box1. Mechanisms of oedema
Presentation
Any patient who presents with unilateral leg swelling should be assessed with the possibility of deep vein thrombosis (DVT) in mind. The pain and swelling of a DVT is often fairly gradual in onset, over hours or even days. Sudden-onset pain in the posterior aspect of the leg is more consistent with gastrocnemius muscle tear (which may be traumatic or spontaneous) or a ruptured Baker's cyst. Leg swelling and pain associated with paraesthesia or paresis, or in the context of lower limb injury or reduced conscious level, should always prompt concern regarding the possibility of compartment syndrome (Box 2).

Box2. Identification of compartment syndrome
Clinical assessment
Lower limb DVT characteristically starts in the distal veins, causing an increase in temperature of the limb and dilatation of the superficial veins. Often, however, symptoms and signs are minimal.
Cellulitis is usually characterised by erythema and skin warmth localised to a well-demarcated area of the leg and may be associated with an obvious source of entry of infection (e.g. leg ulcer or insect bite). The patient may be febrile and systemically unwell. Superficial thrombophlebitis is more localised; erythema and tenderness occur along the course of a firm, palpable vein.
Examination of any patient presenting with leg swelling should include assessment for malignancy (evidence of weight loss, a palpable mass or lymphadenopathy). Malignancy is a risk factor for DVT, but pelvic or lower abdominal masses can also produce leg swelling by compressing the pelvic veins or lymphatics. Early lymphoedema is indistinguishable from other causes of oedema. More chronic lymphoedema is firm and non-pitting, often with thickening of the overlying skin, which may develop a ‘cobblestone’ appearance.
Chronic venous insufficiency is a cause of long-standing oedema that, particularly when combined with another cause of leg swelling, may acutely worsen. Characteristic skin changes (haemosiderin deposition, hair loss, varicose eczema, ulceration) and prominent varicosities are common, and sometimes cause diagnostic confusion with cellulitis. See Box 2 for the examination findings associated with compartment syndrome.
Initial investigations
Clinical criteria can be used to rank patients according to their likelihood of DVT, by using scoring systems that determine pre-test probability, such as the Wells score (Box 3). Figure 1 gives an algorithm for investigation of suspected DVT based on initial Wells score. In patients with a low (‘unlikely’) pre-test probability of DVT, D-dimer levels can be measured; if these are normal, further investigation for DVT is unnecessary. Further information on the interpretation of D-dimer is given in Box4. In those with a moderate or high (‘likely’) probability of DVT or with elevated D-dimer levels, objective diagnosis of DVT should be obtained using appropriate imaging, usually a Doppler ultrasound scan. Therefore, in the same way as for pulmonary embolus, the investigative pathway for DVT differs according to the pre-test probability of DVT. For low-probability DVT, the negative predictive value of the D-dimer test (the most important parameter in this context) is over 99%; if the test is negative, the clinician can discharge the patient with confidence. In patients with a high probability of DVT, the negative predictive value of a D-dimer test falls to somewhere in the region of 97%–98%. While this may initially appear to be a high figure, to discharge 2 or 3 patients in every 100 incorrectly would generally be considered an unacceptable error rate. Hence, with the exception of pregnancy (Box5), a combination of clinical probability and blood test results should be used in the diagnosis of DVT. If cellulitis is suspected, serum inflammatory markers, skin swabs and blood cultures should be sent, ideally before antibiotics are given. Ruptured Baker's cyst and calf muscle tear can both be readily diagnosed on ultrasound. If pelvic or lower abdominal malignancy is suspected, a prostate-specific antigen (PSA) level should be measured in males and appropriate imaging with ultrasound (transabdominal or trans vaginal) or CT should be undertaken.
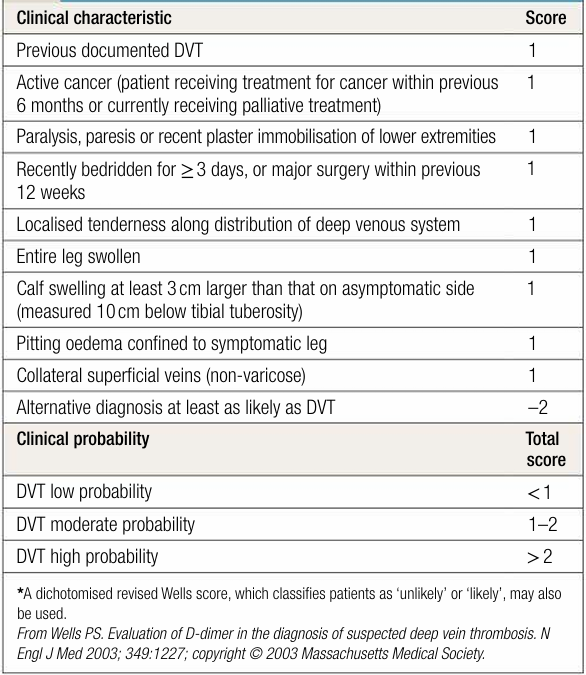
Box3. Predicting the pre-test probability of deep vein thrombosis (DVT) using the Wels score *
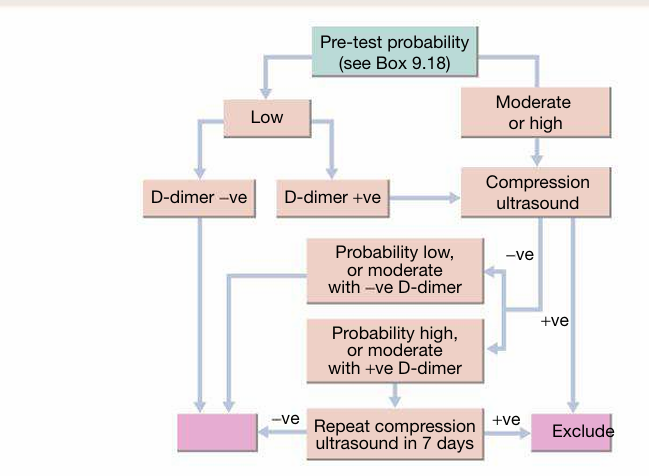
Fig1. Investigation of suspected deep vein thrombosis.
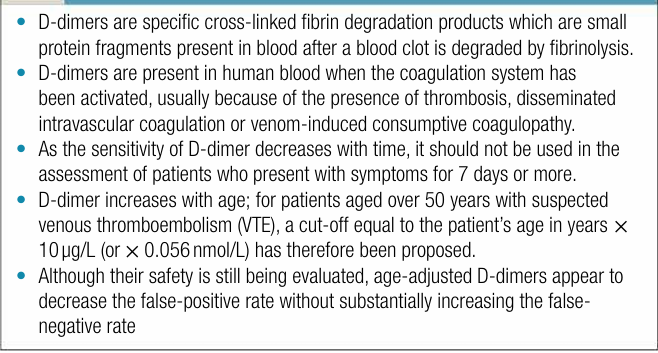
Box4. D-dimer
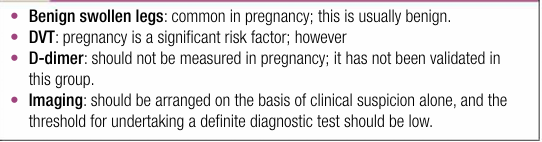
Box5. Swolen legs in pregnancy Treat



|
|
|
|
التوتر والسرطان.. علماء يحذرون من "صلة خطيرة"
|
|
|
|
|
|
|
مرآة السيارة: مدى دقة عكسها للصورة الصحيحة
|
|
|
|
|
|
|
نحو شراكة وطنية متكاملة.. الأمين العام للعتبة الحسينية يبحث مع وكيل وزارة الخارجية آفاق التعاون المؤسسي
|
|
|