آخر المواضيع المضافة

 النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية
النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية| Chromosomal disorders |


|
|
Read More
Date: 19-2-2016
Date: 21-2-2016
Date: 19-2-2016
|
Chromosomal disorders (Cytogenetic disorders)
- are caused by chromosome & genome mutations ( i.e. abnormal structure & number of chromosomes respectively).
- are not uncommon. They are found in 50% of early spontaneous abortuses, in 5% of stillbirths, & in 0.5 -1% of live born infants.
- may, therefore, be suspected in the following clinical situations:
o Spontaneous abortion
o Stillbirth
o Abnormal live births
o Infertile couple
The following subtopics will be discussed below:
A. Normal karyotype
- Chromosome identification & nomenclature
B. Types of chromosomal abnormalities
C. Abnormalities of autosomal chromosomes
E.g. Down syndrome
D. Abnormalities of sex chromosomes
E.g. 1. Klinefelter syndrome
E.g. 2. Turner syndrome
A. The normal karyotype
Chromosome classification & nomenclature:
Karyotype is the chromosome constitution of an individual. The term is also used for a photomicrograph of the chromosomes of an individual arranged in the standard classification (i.e. metaphase chromosomes arranged in order of decreasing length). Karyotyping means the process of preparing such a photomicrograph. I.e. it is the study of chromosomes. Karyotyping uses many types of techniques of which G-banding is the most common procedure.
G-banding has the following steps:-
- Arrest dividing cells in metaphase by using colchicine.
- Stain the metaphase chromosomes using Giemsa stain, hence thename G-banding.→The metaphase chromosomes will show alternating dark staining & light- staining bands. The dark bands are by convention called G bands, & the light bands are R bands. About 400 -800 dark & light bands can be seen in a haploid set of chromosomes using G banding.
- Each chromosome can be identified based on its banding pattern & length. The chromosome pairs are arranged in decreasing order of their length. And the first chromosome in such an arrangement is called chromosome 1, the 2nd chromosome is called chromosome 2, etc…. up to chromosome 23. The banding can also identify breakpoints & other chromosomal alterations.
Metaphase chromosomes are divided longitudinally into 2 sister chromatids held together at the centromere, which delineates the chromosome into a short arm (p) & a long arm (q).
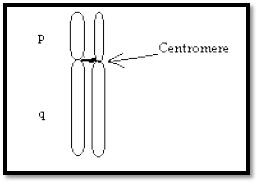
Fig. 1. A pair of chromosomes.
The position of the centromere is used in the morphologic description of a chromosome: Metacentric chromosomes have more central centromeres.
Acrocentric chromosomes have a centromere that is very close to one end. E.g. chromosomes 13 & 21.
In a banded karyotype, each arm of the chromosome is divided into 2 or more regions. The regions are numbered e.g. 1, 2, and 3 from the centromere progressing to the telomere. Each region is further subdivided into bands & sub bands which are also similarly numbered. Thus, Xq22.1 refers to a segment located on the long arm of the X chromosome in region 2 band 2, sub band 1. The following figure illustrates this.

Fig. 2. Nomenclature of a chromosome showing the division of the long arm (q) of the chromosome into regions 1 & 2. Region 2 is further subdivided into bands 1 & 2. Band 2 is further subdivided into sub bands 1 & 2. Even though not shown in this figure, the other bands of this q arm & the p arm are similarly divided & numbered.
Karyotypes are usually described using a shorthand system of notations. The following order is used to describe karyotypes:
- First the total number of chromosomes is given.
- Second the sex chromosome constitution is given.
- Finally any abnormality is described.
E.g. 1. A normal female karyotype is 46,XX. E.g. 2. A female with trisomy 21 is described as 47,XX,+21.
B. Types of chromosomal anomalies
- Chromosomal anomalies may be numerical or structural.
1. Numerical anomalies can result in either aneuploidy or polyploidy.
i. Aneuploidy
- is addition or loss of 1 or rarely 2 chromosomes.
ii. Polyploidy
- is the addition of complete haploid sets of chromosomes.
2. Structural anomalies are rearrangements of genetic material within or between chromosomes. These may be either genetically balanced or unbalanced. In balanced structural anomalies, there is no change in the amount of essential genetic material whereas in the unbalanced ones there is a gain or loss of essential chromosome segments.
1. Numerical anomalies
a. Aneuploidy
- is a chromosome number that is not an exact multiple of 23 (i.e. the normal haploid number). The most common forms of aneuploidy are trisomy & monosomy. Trisomy is the presence of 3 copies of a particular chromosome instead of the normal 2 copies.
I.e. it is the presence of an extra chromosome. Monosomy is the presence of only one copy of a particular chromosome instead of the normal pair. I.e. it is the absence of a single chromosome.
- is caused most often by an addition or loss of 1 or 2 chromosomes. This change may result from anaphase lag or nondisjunction.
i. Anaphase lag
- During meiosis or mitosis, one chromosome lags behind & is left out of the cell nucleus. This results in one normal cell & one cell with monosomy.
ii. Nondisjunction
- is the failure of chromosomes to separate during meiosis or mitosis. The following figure illustrates meiotic nondisjunction.

Fig.3. (A) Normal disjunction of a chromosome pair during meiosis I & II. (B) In meiosis I nondisjunction, the homologous chromosomes fail to segregate into the 2 daughter cells. (C) In meiosis II nondisjunction, the sister chromatids fail to segregate. The chromosome number in the gametes, which in humans is 23, is denoted by n. As shown in this figure both (B) & (C) produce gametes that are disomic or nullisomic for a specific chromosome. And fertilization of such gametes results in trisomic or monosomic zygotes (i.e. aneuploid zygotes). Meiotic nondisjunction is the most common cause of aneuploidy. It is responsible for disorders such as trisomy 21, the most common form of Down syndrome.
Nondisjunction can also occur in a mitotic division of somatic cells after the formation of the zygote. Mitotic nondisjunction is the failure of sister chromatids to segregate at anaphase (like the meiosis II error shown above). If mitotic nondisjunction occurs at an early stage of embryonic development, then clinically significant mosaicism may result. See the following figure.
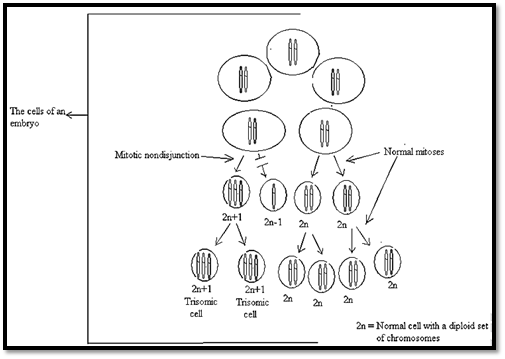
Fig.4. Mitotic nondisjunction at an early stage of development of an embryo.
The mitotic nondisjunction occurred in one of cells & resulted in a trisomic cell. All the descendants of this trisomic cell will also be trisomic. Also note that most of the cells undergo normal mitosis resulting in normal cells. Therefore, an individual formed from such an embryo will have 2 populations of cells – a trisomic cell population & a normal cell population. Such an individual is called a mosaic. And the clinical appearance of such an individual depends on the proportion of trisomic cells. Anyway, the clinical feature is less severe than that of an individual in whom all the cells are trisomic.
In general, monosomies & trisomies of the sex chromosomes are compatible with life & usually cause phenotypic abnormalities. But monosomies & trisomies of the autosomal chromosomes are not well tolerated. I.e. monosomies of autosomal chromosomes are lethal to the conceptus. And trisomies of all autosomal chromosomes except chromosomes 13, 18, & 21 cause abortion or early death. However, trisomies of the autosomal chromosomes, 13, 18, & 21 permit survival with phenotypic abnormalities.
b. Polyploidy
- is a chromosome number that is a multiple greater than 2 of the haploid number. Triploidy is 3x the haploid number (i.e.69 chromosomes).Tetraploidy is 4x.
- is rarely compatible with life & usually results in spontaneous abortion.
2. Structural anomalies
- result from breakage of chromosomes followed by loss or rearrangement of genetic material
- are of the following types (See Fig.5 below):
i. Deletion
- is loss of a portion of a chromosome.
- has the following subtypes (See Fig. 5):-
a. Terminal deletions arise from one break. The acentric fragments that are formed are lost at the next cell division. This is denoted by using the prefix ‘del’ before the notation for the site of the deletion. E.g. 46,XX, del (18)(p14) or it can also be denoted by a minus sign following the number of the chromosome & the sign for the chromosomal arm involved. E.g. 46,XX, 5p- (which indicates deletion of the short arm of chromosome 5)
b. Interstitial deletions arise from 2 breaks, loss of the interstitial acentric segment & fusion at the break sites.
c. Ring chromosomes arise from breaks on either side of the centromere & fusion at the breakpoints on the centric segment. Segments distal to the breaks are lost so that individuals with chromosome rings have deletions from both the long arm & short arm of the chromosome involved. May be denoted as for example 46,XX, r(15).
ii. Isochromosome formation
- results when one arm of a chromosome is lost & the remaining arm is duplicated, resulting in a chromosome consisting of 2 short arms only or 2 long arms only. The arm on one side of the centromere is a mirror image of the other. E.g. i(X)(q10) results in monosomy of the genes on the short arm of X & trisomy of the genes on the long arm of X. (See Fig.5)
iii. Inversion
- is reunion of a chromosome broken at 2 points, in which the internal segment is reinserted in an inverted position.
- are compatible with normal development.
iv. Translocation.
- is an exchange of chromosomal segments between 2 non-homologous chromosomes.
- is denoted by a “t” followed by the involved chromosomes in numerical order.
E.g. the translocation form of Down’s syndrome is designated as t(14q;21q).
- has 2 types (See Fig. 5):
a. Reciprocal (balanced translocation)
- is a break in 2 chromosomes leading to an exchange of chromosomal material between the two chromosomes. Since no genetic material is lost, balanced translocation is often clinically silent. But it can also cause disease as in the t(9,22) which causes chronic myelogenous leukaemia.
b. Robertsonian translocation
- is a variant in which the long arms of 2 acrocentric chromosomes are joined with a common centromere, & the short arms are lost.
Before going into the discussion of some of the chromosomal disorders, it is good to remember what mosaicism is.
Mosaicism
- is the presence of 2 or more cell lines with different karyotypes in a single individual. In a mosaic individual, a normal diploid cell commonly coexists with an abnormal cell line.
The abnormal cell line may have a numerical or structural anomaly. A specific cell line may be represented in all tissues or may be confined to single or multiple tissues. The expression of the phenotype depends on the proportion & distribution of the abnormal cell line.
- is caused by mitotic errors in early development (i.e. in the fertilized ovum/embryo). (See above).

Fig. 5. Types of structural anomalies (structural rearrangements) of chromosomes.
C. Cytogenetic disorders involving autosomes
- include:
o Down syndrome
o Edward syndrome
o Patau syndrome
o Chromosome 22q11 deletion syndrome
Down syndrome
- is the most frequent chromosomal disorder.
- is caused by:-
1. Trisomy 21
- accounts for 95% of cases & its incidence increases with maternal age.
- is produced usually (i.e. in 95% of cases of trisomy) by maternal meiotic nondisjunction. When the cause is paternal nondisjunction, there is no relation to paternal age.
2. Translocation
- accounts for 4% of all cases of Down’s syndrome.
- has no relation to maternal age.
- is caused by paternal meiotic robertsonian translocation between chromosome 21 & another chromosome. The fertilized ovum will have 3 chromosomes bearing the chromosome 21 material, the functional equivalent of trisomy 21.
- leads to a familial form of Down’s syndrome, with a significant risk of the syndrome in subsequent children
3. Mosaicism
- accounts for 1% of cases.
- usually shows a mixture of cells with 46 & 47 chromosomes.
- results from mitotic nondisjunction of chromosome 21 during an early stage of embryogenesis.
- has milder symptoms depending on the proportion of the abnormal cells.
- is not influenced by maternal age.
Down syndrome
- has the following clinical features:
o Severe mental retardation
o Broad (flat) nasal bridge & oblique palpebral fissure. Because of these features
the old name of this disease is mongolism.
o Epicanthic folds
o Wide-spaced eyes
o Large protruding tongue
o Small low-set ears
o Bruschfield’s spots (small white spots in the periphery of the iris).
o Short broad hands with curvature of the 5th
finger, simian crease (a single palmar crease)
o Unusually wide space between the 1st & the 2nd toes
o Congenital heart disease (in about 40% of the cases).
o A 10 – 20 fold increased risk of developing acute leukaemia.
o Increased susceptibility to infection
o In patients surviving to middle age, morphologic changes similar to Alzheimer’s disease.
D. Cytogenetic disorders involving sex chromosomes
The following subtopics will be discussed below:
1. General features
2. Klinefelter syndrome
3. Turner syndrome
4. Disorders of sexual differentiation
1. General features
Sex chromosomal disorders have the following general features:
a. They generally induce subtle, chronic problems relating to sexual development & fertility.
b. They are often difficult to diagnose at birth & many are first recognized at the time of puberty.
c. The higher the number of the X chromosomes (both males & females), the higher the likelihood of mental retardation.
d. They are far more common than those related to autosomal aberrations.
e. They are better tolerated than autosomal disorders. I.e. extreme karyotype deviations in the sex chromosomes are compatible with life. This is due to the following 2 factors that are unique to the sex chromosomes:
i. The scant genetic information carried by the Y chromosome &
ii. The lyonization of the X chromosomes
i. The scant genetic information carried by the Y chromosome:
Most of the Y chromosome appears to be “junk DNA” i.e. repetitive sequences that are without function. But there are some essential genes on the Y chromosome such as the genes which determine the testes, spermatogenesis, etc…. The Y chromosome is both necessary & sufficient for male development. Regardless of the number of the X chromosomes, the presence of a single Y chromosome leads to the male sex.
ii. The lyonization of the X chromosomes (X chromosome inactivation) In normal female somatic cells, there are 2 X chromosomes, but most of the genes on one of the X chromosomes are inactive. The process by which this occurs is called X chromosome inactivation or lyonization or Lyon’s hypothesis.
a. The X chromosome with most of the genes turned off is called the inactive X chromosome. The other one is called the active X chromosome.
b. If a somatic cell contains more than one X chromosome, all but one are inactivated. E.g.1. In a 47, XXY cell, there is one active & one inactive X chromosome (the Y chromosome is irrelevant to the process of X inactivation). E.g. 2 in a 49, XXXXX cell, there is one active X chromosome & 4 inactive chromosomes
c. X inactivation occurs early in embryogenesis among all cells of the bastocyst at about the 16th day of embryonic life.
d. The process of X inactivation is random in any single cell. Either the X chromosome inherited from the mother (called Xm) or the X chromosome inherited from the father (called Xp) may be inactivated with equal likelihood.
e. Once X inactivation occurs in an embryonic cell, the same X chromosome remains inactivated in all of the progeny of that cell. Females are mosaics. On average, half of the cells in a female have an inactive Xm & the other half of the cells have an inactive Xp. However, some tissues (& some women ) may have substantially more cells with one or the other X chromosome active by chance.
f. X inactivation involves most, but not all, genes on the X chromosome. Some essential genes must be expressed in 2 copies from both X chromosomes for normal growth & development. For this reason, some essential genes on the X chromosome escape X-inactivation. So if one of these essential genes is absent (as occurs in Turner syndrome), it results in abnormal growth & development. Likewise, the presence of an extra X chromosome (as occurs in Klinefelter syndrome) leads to abnormal phenotype.
g. The inactive X-chromosome may be visible in an interphase cell as a condensed mass of chromatin called the Barr body (X chromatin). The maximum number of Barr bodies seen in a cell is equal to the number of inactivated X chromosomes (i.e. one less than the total number of X chromosomes in the cell). E.g. Normal females (46,XX) will have one Barr body, & individuals with 3 chromosomes (XXX) will have 2 Barr bodies, & those with 4 X chromosomes will have 3, & so on. Counting the number of Barr bodies in somatic cells (usually in smears of buccal mucosa) is the basis of the sex chromatin test for sex chromatin aneuplody. This test is no longer used in the Western countries because karyotyping is much more accurate.
h. X-chromosome inactivation produces dosage compensation. Females normally have 2 X-chromosomes & males have only one. And most of the genes on the X chromosome do not have homologues on the Y chromosome. Despite the fact that females have double doses of most X-linked genes in comparison to males, the amount of X –linked products is usually about the same in males & females. This dosage compensation is produced by X inactivation.
i. X inactivation has the following clinical implications:
1. A female who carries an X-linked recessive mutation on one of her 2 X chromosomes may express the mutant phenotype if most of her cells happen to have inactivated the X chromosome carrying the normal gene.
2. A female carrier of an X-linked recessive disease may not detectable by gene product assays (e.g. by the amount of protein or enzyme activity) if most of her cells happen to inactivate the X chromosome carrying the mutant gene.
3. Although monosomy (i.e. the presence of one instead of the normal 2 copies) for any autosome is lethal early in embryogenesis; monosomy for the X chromosome is relatively common in live born infants & produces a relatively mild phenotype called Turner syndrome.
4. Trisomy (i.e. the presence of 3 rather than the normal 2 copies) of the sex chromosomes produces a much less severe phenotype than trisomy for any of the autosomes. Trisomy of the sex chromosomes produces phenotypic changes because of the triple dosage of the essential genes on the X chromosomes (1 copy of these essential genes on the active X chromosome & 2 copies of the activated ‘escapee’ essential genes on the inactivated X chromosome). Points 3 & 4 above illustrate that aneuploidy of the sex chromosomes is better tolerated than the aneuploidy of the autosomes.
2. Klinefelter syndrome
- is a disorder that occurs when there are at least 2 X chromosomes & 1 or more Y chromosomes.
- is most often characterized by the karyotype 47, XXY. Variants include additional X chromosomes (e.g. XXXY) & rare mosaic forms. In the typical XXY form, a single Barr body is noted in the buccal smear preparations.
- is caused by parental meiotic nondisjunction & incidence increases with maternal age.
- is characterized by male hypogonadism & its secondary effects.
- shows atrophic testes with decreased spermatogenesis which leads to infertility & decreased testosterone production. In addition, it also shows increased plasma estradiol levels (by unknown mechanism). The ratio of estrogens & testosterone determines the degree of feminization.
- therefore, shows lack of secondary male sexual characteristics (i.e. no deep voice, no beard, no male distribution of pubic hair).
- also shows tall stature (because fusion of the epiphyses is delayed), & eunuchoid appearance with gynecomastia.
- is rarely associated with mental retardation, which is usually mild. The extent of retardation increases with increased number of X chromosomes.
- is usually undiagnosed before puberty.
3. Turner syndrome
- is a disorder that occurs when there is a complete or partial monosomy of the X chromosome.
- is associated with one of the following 3 types of karyotypic abnormalities:
o 45,X karyotype ( in which no Barr bodies are seen in the buccal smear)
o mosaics (45, X cell plus one or more karyotypically normal or abnormal cell types)
o structural abnormalities of the X chromosomes which result in partial monosomy of the X chromosome. E.g. deletion of one of the arms of the X chromosome.
This karyotypic heterogeneity associated with Turner’s syndrome is responsible for significant variations in phenotype. E.g. 45, XO causes a severe phenotype whereas mosaics may have a normal appearance with only primary amenorrhea.
- is characterized by female hypogonadism & its secondary effects.
- shows:-
o Replacement of the ovaries by fibrous streaks .
o Decreased estrogen production & increased pituitary gonadotropins from loss of feedback inhibition.
o Infantile genitalia & poor breast development & little pubic hair.
o Short stature (rarely exceeding 150cm in height), webbed neck, shield-like chest with widely spaced nipples, & wide carrying angles of the arms.
o Lymphedema of the extremities & neck.
o Congenital heart disease (especially preductal coarctation of the aorta & bicuspid aortic valve).
4. Disorders of sexual differentiation (Sexual ambiguity)
- are said to be present when genetic sex, gonadal sex, or genital sex of an individual are discordant.
i. Definitions
The sex of an individual can be defined on many levels:-
1. Genetic sex
- is determined by the presence or absence of a Y chromosome. No matter how many X chromosomes are present, the presence of a single Y chromosome leads to testicular development & a genetic male. At least one Y chromosome is necessary & sufficient for male gender to manifest.
2. Gonadal sex
- is determined by the presence of ovaries or testes. The gene responsible for the development of the testes is localized to the Y chromosome.
3. Ductal sex
- depends on the presence of derivatives of the Mullerian or Wolffian ducts.
4. Phenotypic or genital sex
- is based on the appearance of the external genitalia.
Sexual ambiguity is present whenever there is discordance among these various criteria for determining sex.
ii. True hermaphrodite
- is very rare.
- has both ovaries & testicular tissue, with ambiguous external genitalia.
- may result from the fusion of 2 sperms (one X-carrying sperm & one Y-carrying sperm) with a binucleated ovum.
iii. Pseudohermaphrodite
- shows discordance between the phenotypic sex & gonadal sex.
- i.e. has gonads of only one sex, but the appearance of the external genitalia does not correspond to the gonads present. Thus, a male pseudohermaphrodite has testicular tissue but female-type genitalia. A female pseudohermaphrodite has a ovaries but male external genitalia (or the external genitalia are not clearly male).
1. Female pseudohermaphroditism
- is caused by exposure of the fetus to increased androgenic hormones during the early part of gestation as occurs in congenital adrenal hyperplasia, androgen-secreting ovarian or adrenal tumor in the mother, or hormones administered to the mother during pregnancy.
2. Male pseudohermaphroditism
- has a Y chromosome & only testes but the genital ducts or the external genitalia are either ambiguous or completely female.
- may be caused by tissue resistance to androgens (called testicular feminization), by defects in testosterone synthesis, or by estrogens administered to the mother during pregnancy.
References
Bezabeh ,M. ; Tesfaye,A.; Ergicho, B.; Erke, M.; Mengistu, S. and Bedane,A.; Desta, A.(2004). General Pathology. Jimma University, Gondar University Haramaya University, Dedub University.



|
|
|
|
تفوقت في الاختبار على الجميع.. فاكهة "خارقة" في عالم التغذية
|
|
|
|
|
|
|
أمين عام أوبك: النفط الخام والغاز الطبيعي "هبة من الله"
|
|
|
|
|
|
|
قسم شؤون المعارف ينظم دورة عن آليات عمل الفهارس الفنية للموسوعات والكتب لملاكاته
|
|
|